Looking At Pes Planus
Overview

Our feet are incredibly well specialized structures. There are 26 different bones in each foot, held together by 33 joints and more than 100 muscles, tendons and ligaments (in each foot). They way they weave and align together determine the formation of our arches. The aim of the arches is to give us spring and distribute our body weight across our feet and legs. The structures of the arches of our feet determine how we walk - they are rigid levels which allow us to move smoothly. However, the arches need to be sturdy as well as flexible to adapt to various surfaces and stresses. During childhood it is normal to have flat feet. This is because our feet form during our childhood. In other words, having what appears to be flat feet during early childhood does not necessarily mean that it will persist throughout the individual's life. People with very low arches or what appear to be no arches at all may experience no problems.
Causes
Flat feet are often a congenital problem which has no specific cause. They can however occur after an injury, especially conditions such as Tibialis Posterior Syndrome or more traumatic injuries such as fractures or mid-tarsal joint sprains. The other thing to look out for is Overpronation. Often this is confused with having flat feet (or a fallen arch) although it is not technically the same thing. If an individual does not have flat feet but does overpronate then the arch of their foot appears to be normal when standing. However, when they walk the arch collapses and the foot rolls in excessively. This is more difficult to spot than flat feet. It is estimated that between 60 and 80% of the population overpronate!
Symptoms
Symptoms that should be checked by a pediatrician include foot pain, sores or pressure areas on the inner side of the foot, a stiff foot, limited side-to-side foot motion, or limited up-and-down ankle motion. For further treatment you should see a pediatric orthopedic surgeon or podiatrist experienced in childhood foot conditions.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
Why do arches fall?
Non Surgical Treatment
Flexible flat feet that are painless do not require treatment. If you have pain due to flexible flat feet, an orthotic (arch-supporting insert in the shoe) can bring relief. With the increased interest in running, many shoe stores carry shoes for normal feet and pronated feet. The shoes designed for pronated feet make long distance running easier and less tiring because they correct for the abnormality. Rigid or painful flat feet require evaluation by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. If this fails to improve the pain, surgery may be necessary. For problems with the posterior tibial tendon, treatment may start with rest, anti-inflammatory medications, and shoe inserts or ankle braces. In more advanced cases, surgery may be needed to clean or repair the tendon, or fuse some of the joints of the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment

Rarely does the physician use surgery to correct a foot that is congenitally flat, which typically does not cause pain. If the patient has a fallen arch that is painful, though, the foot and ankle physicians at Midwest Orthopaedics at Rush may perform surgery to reconstruct the tendon and "lift up" the fallen arch. This requires a combination of tendon re-routing procedures, ligament repairs, and bone cutting or fusion procedures.
Our feet are incredibly well specialized structures. There are 26 different bones in each foot, held together by 33 joints and more than 100 muscles, tendons and ligaments (in each foot). They way they weave and align together determine the formation of our arches. The aim of the arches is to give us spring and distribute our body weight across our feet and legs. The structures of the arches of our feet determine how we walk - they are rigid levels which allow us to move smoothly. However, the arches need to be sturdy as well as flexible to adapt to various surfaces and stresses. During childhood it is normal to have flat feet. This is because our feet form during our childhood. In other words, having what appears to be flat feet during early childhood does not necessarily mean that it will persist throughout the individual's life. People with very low arches or what appear to be no arches at all may experience no problems.
Causes
Flat feet are often a congenital problem which has no specific cause. They can however occur after an injury, especially conditions such as Tibialis Posterior Syndrome or more traumatic injuries such as fractures or mid-tarsal joint sprains. The other thing to look out for is Overpronation. Often this is confused with having flat feet (or a fallen arch) although it is not technically the same thing. If an individual does not have flat feet but does overpronate then the arch of their foot appears to be normal when standing. However, when they walk the arch collapses and the foot rolls in excessively. This is more difficult to spot than flat feet. It is estimated that between 60 and 80% of the population overpronate!
Symptoms
Symptoms that should be checked by a pediatrician include foot pain, sores or pressure areas on the inner side of the foot, a stiff foot, limited side-to-side foot motion, or limited up-and-down ankle motion. For further treatment you should see a pediatric orthopedic surgeon or podiatrist experienced in childhood foot conditions.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
Why do arches fall?
Non Surgical Treatment
Flexible flat feet that are painless do not require treatment. If you have pain due to flexible flat feet, an orthotic (arch-supporting insert in the shoe) can bring relief. With the increased interest in running, many shoe stores carry shoes for normal feet and pronated feet. The shoes designed for pronated feet make long distance running easier and less tiring because they correct for the abnormality. Rigid or painful flat feet require evaluation by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. If this fails to improve the pain, surgery may be necessary. For problems with the posterior tibial tendon, treatment may start with rest, anti-inflammatory medications, and shoe inserts or ankle braces. In more advanced cases, surgery may be needed to clean or repair the tendon, or fuse some of the joints of the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment
Rarely does the physician use surgery to correct a foot that is congenitally flat, which typically does not cause pain. If the patient has a fallen arch that is painful, though, the foot and ankle physicians at Midwest Orthopaedics at Rush may perform surgery to reconstruct the tendon and "lift up" the fallen arch. This requires a combination of tendon re-routing procedures, ligament repairs, and bone cutting or fusion procedures.
Heel Pain
Overview

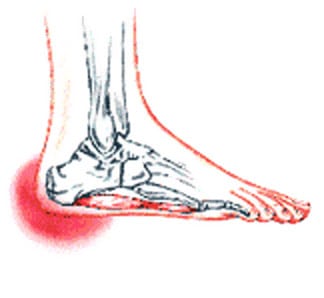
Heel pain is pain in the heel area that can vary in severity and location. It is most common in adults. The heel is the first bone to contact the ground when walking and takes the full force of impact and the resulting shock of bearing weight during motion.
Causes
To understand the cause of the pain one must understand the anatomy of the foot and some basic mechanics in the function of the foot. A thick ligament, called the plantar fascia, is attached into the bottom of the heel and fans out into the ball of the foot, attaching into the base of the toes. The plantar fascia is made of dense, fibrous connective tissue that will stretch very little. It acts something like a shock absorber. As the foot impacts the ground with each step, it flattens out lengthening the foot. This action pulls on the plantar fascia, which stretches slightly. When the heel comes off the ground the tension on the ligament is released. Anything that causes the foot to flatten excessively will cause the plantar fascia to stretch greater that it is accustom to doing. One consequence of this is the development of small tears where the ligament attaches into the heel bone. When these small tears occur, a very small amount of bleeding occurs and the tension of the plantar fascia on the heel bone produces a spur on the bottom of the heel to form. Pain experienced in the bottom of the heel is not produced by the presence of the spur. The pain is due to excessive tension of the plantar fascia as it tears from its attachment into the heel bone. Heel spur formation is secondary to the excessive pull of the plantar fascia where it attaches to the heel bone. Many people have heel spurs at the attachment of the plantar fascia with out having any symptoms or pain. There are some less common causes of heel pain but they are relatively uncommon. There are several factors that cause the foot to flatten and excessively stretching the plantar fascia. The primary factor is the structure of a joint complex below the ankle joint, called the subtalar joint. The movement of this joint complex causes the arch of the foot to flatten and to heighten. Flattening of the arch of the foot is termed pronation and heightening of the arch is called supination. If there is excessive pronation of the foot during walking and standing, the plantar fascia is strained. Over time, this will cause a weakening of the ligament where it attaches into the heel bone, causing pain. When a person is at rest and off of their feet, the plantar fascia attempts to mend itself. Then, with the first few steps the fascia re-tears causing pain. Generally, after the first few steps the pain diminishes. This is why the heel pain tends to be worse the first few steps in the morning or after rest. Another factor that contributes to the flattening of the arch of the foot is tightness of the calf muscles. The calf muscle attaches into the foot by the achilles tendon into the back of the heel. When the calf muscle is tight it limits the movement of the ankle joint. When ankle joint motion is limited by the tightness of the calf muscle it forces the subtalar joint to pronate excessively. Excessive subtalar joint pronation can cause several different problems to occur in the foot. In this instance, it results in excessive tension of the plantar fascia. Tightness of the calf muscles can be a result of several different factors. Exercise, such as walking or jogging will cause the calf muscle to tighten. Inactivity or prolonged rest will also cause the calf muscle to tighten. Women who wear high heels and men who wear western style cowboy boots will, over time, develop tightness in the calf muscles.
Symptoms
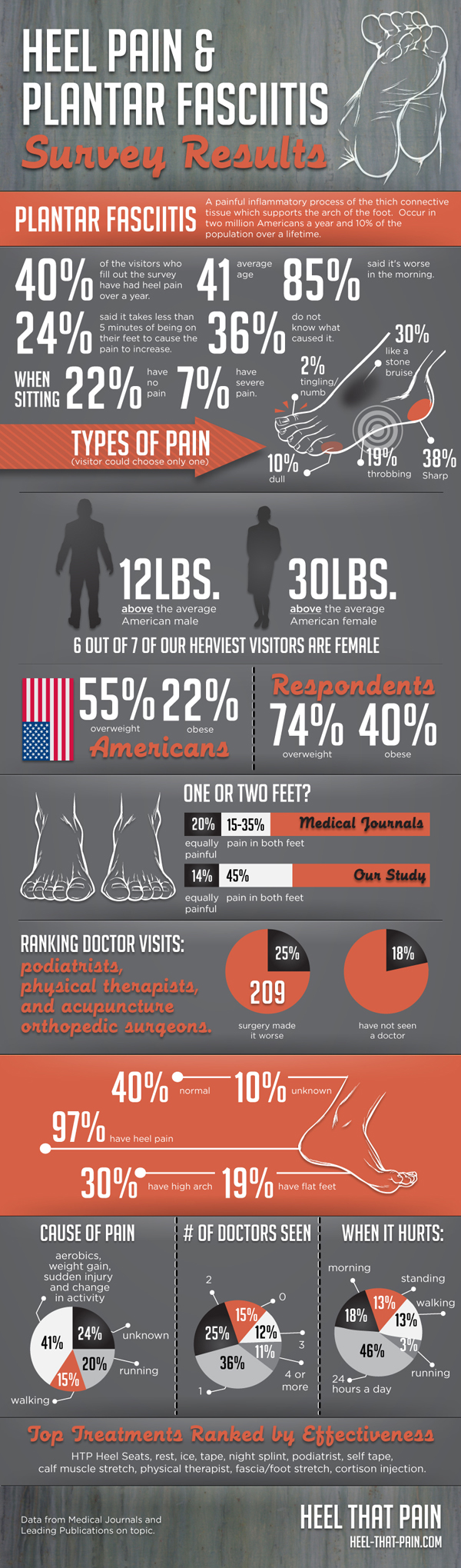
Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, by being overweight. It doesn't help that fascia doesn't heal particularly quickly because it has relatively poor circulation (which is why it's white in colour).
Diagnosis
A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans.
Non Surgical Treatment
Morning Wall Stretch. Stand barefoot in front of wall, as shown. Press into wall with both hands and lean forward, feeling stretch along back of left leg and heel. Hold for 30 seconds; switch sides and repeat. Freeze and Roll. Freeze a small water bottle. Cover it with a towel and place arch of your foot on top of it. Slowly roll bottle beneath arch of foot for about 5 minutes at a time. Switch sides and repeat. Rub It Out. Use both thumbs to apply deep pressure along arch of the feet, heel, and calf muscles, moving slowly and evenly. Continue for 1 minute. Switch sides and repeat. If you foot pain isn't improving or worsens after 2 weeks, a podiatrist or othopedist can prescribe additional therapies to alleviate discomfort and prevent recurrence.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
what does a heel spur look like
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don't underestimate your body's need for rest and good nutrition. If obese, lose weight.
Heel pain is pain in the heel area that can vary in severity and location. It is most common in adults. The heel is the first bone to contact the ground when walking and takes the full force of impact and the resulting shock of bearing weight during motion.
Causes
To understand the cause of the pain one must understand the anatomy of the foot and some basic mechanics in the function of the foot. A thick ligament, called the plantar fascia, is attached into the bottom of the heel and fans out into the ball of the foot, attaching into the base of the toes. The plantar fascia is made of dense, fibrous connective tissue that will stretch very little. It acts something like a shock absorber. As the foot impacts the ground with each step, it flattens out lengthening the foot. This action pulls on the plantar fascia, which stretches slightly. When the heel comes off the ground the tension on the ligament is released. Anything that causes the foot to flatten excessively will cause the plantar fascia to stretch greater that it is accustom to doing. One consequence of this is the development of small tears where the ligament attaches into the heel bone. When these small tears occur, a very small amount of bleeding occurs and the tension of the plantar fascia on the heel bone produces a spur on the bottom of the heel to form. Pain experienced in the bottom of the heel is not produced by the presence of the spur. The pain is due to excessive tension of the plantar fascia as it tears from its attachment into the heel bone. Heel spur formation is secondary to the excessive pull of the plantar fascia where it attaches to the heel bone. Many people have heel spurs at the attachment of the plantar fascia with out having any symptoms or pain. There are some less common causes of heel pain but they are relatively uncommon. There are several factors that cause the foot to flatten and excessively stretching the plantar fascia. The primary factor is the structure of a joint complex below the ankle joint, called the subtalar joint. The movement of this joint complex causes the arch of the foot to flatten and to heighten. Flattening of the arch of the foot is termed pronation and heightening of the arch is called supination. If there is excessive pronation of the foot during walking and standing, the plantar fascia is strained. Over time, this will cause a weakening of the ligament where it attaches into the heel bone, causing pain. When a person is at rest and off of their feet, the plantar fascia attempts to mend itself. Then, with the first few steps the fascia re-tears causing pain. Generally, after the first few steps the pain diminishes. This is why the heel pain tends to be worse the first few steps in the morning or after rest. Another factor that contributes to the flattening of the arch of the foot is tightness of the calf muscles. The calf muscle attaches into the foot by the achilles tendon into the back of the heel. When the calf muscle is tight it limits the movement of the ankle joint. When ankle joint motion is limited by the tightness of the calf muscle it forces the subtalar joint to pronate excessively. Excessive subtalar joint pronation can cause several different problems to occur in the foot. In this instance, it results in excessive tension of the plantar fascia. Tightness of the calf muscles can be a result of several different factors. Exercise, such as walking or jogging will cause the calf muscle to tighten. Inactivity or prolonged rest will also cause the calf muscle to tighten. Women who wear high heels and men who wear western style cowboy boots will, over time, develop tightness in the calf muscles.
Symptoms
Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, by being overweight. It doesn't help that fascia doesn't heal particularly quickly because it has relatively poor circulation (which is why it's white in colour).
Diagnosis
A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans.
Non Surgical Treatment
Morning Wall Stretch. Stand barefoot in front of wall, as shown. Press into wall with both hands and lean forward, feeling stretch along back of left leg and heel. Hold for 30 seconds; switch sides and repeat. Freeze and Roll. Freeze a small water bottle. Cover it with a towel and place arch of your foot on top of it. Slowly roll bottle beneath arch of foot for about 5 minutes at a time. Switch sides and repeat. Rub It Out. Use both thumbs to apply deep pressure along arch of the feet, heel, and calf muscles, moving slowly and evenly. Continue for 1 minute. Switch sides and repeat. If you foot pain isn't improving or worsens after 2 weeks, a podiatrist or othopedist can prescribe additional therapies to alleviate discomfort and prevent recurrence.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
what does a heel spur look like
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don't underestimate your body's need for rest and good nutrition. If obese, lose weight.
Leg Length Discrepancy Weight Lifting
Overview
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Causes
A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences.
Symptoms
The effects vary from patient to patient, depending on the cause of the discrepancy and the magnitude of the difference. Differences of 3 1/2 to 4 percent of the total length of the lower extremity (4 cm or 1 2/3 inches in an average adult), including the thigh, lower leg and foot, may cause noticeable abnormalities while walking and require more effort to walk. Differences between the lengths of the upper extremities cause few problems unless the difference is so great that it becomes difficult to hold objects or perform chores with both hands. You and your physician can decide what is right for you after discussing the causes, treatment options and risks and benefits of limb lengthening, including no treatment at all. Although an LLD may be detected on a screening examination for curvature of the spine (scoliosis), LLD does not cause scoliosis. There is controversy about the effect of LLD on the spine. Some studies indicate that people with an LLD have a greater incidence of low back pain and an increased susceptibility to injuries, but other studies refute this relationship.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
A properly made foot orthotic can go a long way in substituting additional millimeters or centimeter on the deficient side. Additional full length inserts are added to the shorter side bringing the runner closer to symmetrical. Heel lifts do not work in runners because when you run you may land on your heel but the rest of the time you are on your forefoot then your toes pushing off. The right custom-made, biomechanical orthotic can address the underlying cause of your pain. Abnormal joint position, overpronation or foot rigidity can be addressed and the biomechanics normalized. San Diego Running Institute orthotics are custom molded to your foot and are designed with your specific body weight, leg length discrepancy, and activity in mind. The restoration of correct mechanical function takes the abnormal stress from the uneven side and allows the body to heal naturally.

how to grow taller fast in a week
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Causes
A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences.
Symptoms
The effects vary from patient to patient, depending on the cause of the discrepancy and the magnitude of the difference. Differences of 3 1/2 to 4 percent of the total length of the lower extremity (4 cm or 1 2/3 inches in an average adult), including the thigh, lower leg and foot, may cause noticeable abnormalities while walking and require more effort to walk. Differences between the lengths of the upper extremities cause few problems unless the difference is so great that it becomes difficult to hold objects or perform chores with both hands. You and your physician can decide what is right for you after discussing the causes, treatment options and risks and benefits of limb lengthening, including no treatment at all. Although an LLD may be detected on a screening examination for curvature of the spine (scoliosis), LLD does not cause scoliosis. There is controversy about the effect of LLD on the spine. Some studies indicate that people with an LLD have a greater incidence of low back pain and an increased susceptibility to injuries, but other studies refute this relationship.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
A properly made foot orthotic can go a long way in substituting additional millimeters or centimeter on the deficient side. Additional full length inserts are added to the shorter side bringing the runner closer to symmetrical. Heel lifts do not work in runners because when you run you may land on your heel but the rest of the time you are on your forefoot then your toes pushing off. The right custom-made, biomechanical orthotic can address the underlying cause of your pain. Abnormal joint position, overpronation or foot rigidity can be addressed and the biomechanics normalized. San Diego Running Institute orthotics are custom molded to your foot and are designed with your specific body weight, leg length discrepancy, and activity in mind. The restoration of correct mechanical function takes the abnormal stress from the uneven side and allows the body to heal naturally.
how to grow taller fast in a week
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Coping with Mortons Neuroma
Overview
 Morton's neuroma is a painful condition that affects the ball of your foot, most commonly the area between your third and fourth toes. Morton's neuroma may feel as if you are standing on a pebble in your shoe or on a fold in your sock. Morton's neuroma involves a thickening of the tissue around one of the nerves leading to your toes. This can cause a sharp, burning pain in the ball of your foot. Your toes also may sting, burn or feel numb. High-heeled shoes have been linked to the development of Morton's neuroma. Many people experience relief by switching to lower heeled shoes with wider toe boxes. Sometimes corticosteroid injections or surgery may be necessary.
Morton's neuroma is a painful condition that affects the ball of your foot, most commonly the area between your third and fourth toes. Morton's neuroma may feel as if you are standing on a pebble in your shoe or on a fold in your sock. Morton's neuroma involves a thickening of the tissue around one of the nerves leading to your toes. This can cause a sharp, burning pain in the ball of your foot. Your toes also may sting, burn or feel numb. High-heeled shoes have been linked to the development of Morton's neuroma. Many people experience relief by switching to lower heeled shoes with wider toe boxes. Sometimes corticosteroid injections or surgery may be necessary.
Causes
It's not always clear what causes Morton's neuroma, but several things seem to aggravate it. These include other foot-related problems and wearing restrictive footwear. It's thought that Morton's neuroma may be caused by the toe bones (metatarsal bones) pressing against the nerve when the gap between the bones is narrow. This causes the nerve and surrounding tissue to thicken.
Symptoms
Feelings of numbness, tingling or tenderness in the ball of the foot (the area just behind the base of the toes) are some of the first signs of a condition known as Morton?s Neuroma. However, the condition is somewhat unpredictable, and symptoms may vary from patient to patient. Generally, however, the discomfort gets worse rather than better, and the patient may feel pain or a burning sensation that radiates out to the toes. Eventually, wearing shoes becomes uncomfortable (or even unbearable), and the patient may complain that the feeling is similar to that of having a stone bruise, or walking on a marble or pebble constantly, even though no there is no trauma to the skin, and no visible bump or lump on the sole of the foot.
Diagnosis
The exact cause of Mortons neuroma can often vary between patients. An accurate diagnosis must be carefully made by the podiatrist through thorough history taking and direct questioning to ensure all possible causes are addressed. The podiatrist will also gather further information about the cause through a hands on assessment where they will try to reproduce your symptoms. A biomechanical and gait analysis will also be performed to assess whether poor foot alignment and function has contributed to your neuroma.
Non Surgical Treatment
Treatment strategies for Morton's neuroma range from conservative to surgical management. The conservative approach to treating Morton's neuroma may benefit from the involvement of a physical therapist. The physical therapist can assist the physician in decisions regarding the modification of footwear, which is the first treatment step. Recommend soft-soled shoes with a wide toe box and low heel (eg, an athletic shoe). High-heeled, narrow, nonpadded shoes should not be worn, because they aggravate the condition. The next step in conservative management is to alter alignment of the metatarsal heads. One recommended action is to elevate the metatarsal head medial and adjacent to the neuroma, thereby preventing compression and irritation of the digital nerve. A plantar pad is used most often for elevation. Have the patient insert a felt or gel pad into the shoe to achieve the desired elevation of the above metatarsal head. Other possible physical therapy treatment ideas for patients with Morton's neuroma include cryotherapy, ultrasonography, deep tissue massage, and stretching exercises. Ice is beneficial to decrease the associated inflammation. Phonophoresis also can be used, rather than just ultrasonography, to further decrease pain and inflammation.
Surgical Treatment
Surgery for neuroma most often involves removing affected nerve in the ball of the foot. An incision is made on the top of the foot and the nerve is carefully removed. Surgeon must remove the nerve far enough back so that the nerve doesn?t continue to become impinged at the ball of the foot. Alternatitvely, another type of surgery involves releasing a tight ligament that encases the nerve. Recovery after Morton?s neuroma (neurectomy) surgery is generally quick. Typically patients are walking on the operated foot in a post-surgical shoe for 2 - 4 weeks, depending on healing. Return to shoes is 2-6 weeks after the surgery. Factors that may prolong healing are age, smoking, poor nutritional status, and some medical problems.
Morton's neuroma is a painful condition that affects the ball of your foot, most commonly the area between your third and fourth toes. Morton's neuroma may feel as if you are standing on a pebble in your shoe or on a fold in your sock. Morton's neuroma involves a thickening of the tissue around one of the nerves leading to your toes. This can cause a sharp, burning pain in the ball of your foot. Your toes also may sting, burn or feel numb. High-heeled shoes have been linked to the development of Morton's neuroma. Many people experience relief by switching to lower heeled shoes with wider toe boxes. Sometimes corticosteroid injections or surgery may be necessary.Causes
It's not always clear what causes Morton's neuroma, but several things seem to aggravate it. These include other foot-related problems and wearing restrictive footwear. It's thought that Morton's neuroma may be caused by the toe bones (metatarsal bones) pressing against the nerve when the gap between the bones is narrow. This causes the nerve and surrounding tissue to thicken.
Symptoms
Feelings of numbness, tingling or tenderness in the ball of the foot (the area just behind the base of the toes) are some of the first signs of a condition known as Morton?s Neuroma. However, the condition is somewhat unpredictable, and symptoms may vary from patient to patient. Generally, however, the discomfort gets worse rather than better, and the patient may feel pain or a burning sensation that radiates out to the toes. Eventually, wearing shoes becomes uncomfortable (or even unbearable), and the patient may complain that the feeling is similar to that of having a stone bruise, or walking on a marble or pebble constantly, even though no there is no trauma to the skin, and no visible bump or lump on the sole of the foot.
Diagnosis
The exact cause of Mortons neuroma can often vary between patients. An accurate diagnosis must be carefully made by the podiatrist through thorough history taking and direct questioning to ensure all possible causes are addressed. The podiatrist will also gather further information about the cause through a hands on assessment where they will try to reproduce your symptoms. A biomechanical and gait analysis will also be performed to assess whether poor foot alignment and function has contributed to your neuroma.
Non Surgical Treatment
Treatment strategies for Morton's neuroma range from conservative to surgical management. The conservative approach to treating Morton's neuroma may benefit from the involvement of a physical therapist. The physical therapist can assist the physician in decisions regarding the modification of footwear, which is the first treatment step. Recommend soft-soled shoes with a wide toe box and low heel (eg, an athletic shoe). High-heeled, narrow, nonpadded shoes should not be worn, because they aggravate the condition. The next step in conservative management is to alter alignment of the metatarsal heads. One recommended action is to elevate the metatarsal head medial and adjacent to the neuroma, thereby preventing compression and irritation of the digital nerve. A plantar pad is used most often for elevation. Have the patient insert a felt or gel pad into the shoe to achieve the desired elevation of the above metatarsal head. Other possible physical therapy treatment ideas for patients with Morton's neuroma include cryotherapy, ultrasonography, deep tissue massage, and stretching exercises. Ice is beneficial to decrease the associated inflammation. Phonophoresis also can be used, rather than just ultrasonography, to further decrease pain and inflammation.
Surgical Treatment
Surgery for neuroma most often involves removing affected nerve in the ball of the foot. An incision is made on the top of the foot and the nerve is carefully removed. Surgeon must remove the nerve far enough back so that the nerve doesn?t continue to become impinged at the ball of the foot. Alternatitvely, another type of surgery involves releasing a tight ligament that encases the nerve. Recovery after Morton?s neuroma (neurectomy) surgery is generally quick. Typically patients are walking on the operated foot in a post-surgical shoe for 2 - 4 weeks, depending on healing. Return to shoes is 2-6 weeks after the surgery. Factors that may prolong healing are age, smoking, poor nutritional status, and some medical problems.
Are Shoe Lifts The Answer To Leg Length Imbalances
There are actually two unique variations of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is structurally shorter compared to the other. As a result of developmental stages of aging, the brain picks up on the stride pattern and recognizes some difference. Our bodies typically adapts by tilting one shoulder to the "short" side. A difference of under a quarter inch isn't grossly irregular, doesn't need Shoe Lifts to compensate and ordinarily won't have a profound effect over a lifetime.

Leg length inequality goes mainly undiscovered on a daily basis, however this issue is simply corrected, and can reduce numerous instances of back pain.
Treatment for leg length inequality commonly involves Shoe Lifts . These are typically economical, typically being below twenty dollars, in comparison to a custom orthotic of $200 and up. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Lumbar pain is easily the most common ailment affecting men and women today. Over 80 million men and women have problems with back pain at some point in their life. It's a problem that costs employers millions every year due to time lost and production. Fresh and superior treatment solutions are constantly sought after in the hope of minimizing the economic impact this issue causes.

Men and women from all corners of the earth suffer the pain of foot ache due to leg length discrepancy. In most of these situations Shoe Lifts might be of very useful. The lifts are capable of relieving any discomfort in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic practitioners".
To be able to support the body in a nicely balanced manner, feet have a very important job to play. Inspite of that, it is sometimes the most neglected area in the body. Some people have flat-feet meaning there may be unequal force placed on the feet. This causes other parts of the body like knees, ankles and backs to be impacted too. Shoe Lifts guarantee that suitable posture and balance are restored.
Leg length inequality goes mainly undiscovered on a daily basis, however this issue is simply corrected, and can reduce numerous instances of back pain.
Treatment for leg length inequality commonly involves Shoe Lifts . These are typically economical, typically being below twenty dollars, in comparison to a custom orthotic of $200 and up. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Lumbar pain is easily the most common ailment affecting men and women today. Over 80 million men and women have problems with back pain at some point in their life. It's a problem that costs employers millions every year due to time lost and production. Fresh and superior treatment solutions are constantly sought after in the hope of minimizing the economic impact this issue causes.
Men and women from all corners of the earth suffer the pain of foot ache due to leg length discrepancy. In most of these situations Shoe Lifts might be of very useful. The lifts are capable of relieving any discomfort in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic practitioners".
To be able to support the body in a nicely balanced manner, feet have a very important job to play. Inspite of that, it is sometimes the most neglected area in the body. Some people have flat-feet meaning there may be unequal force placed on the feet. This causes other parts of the body like knees, ankles and backs to be impacted too. Shoe Lifts guarantee that suitable posture and balance are restored.
What Is The Most Beneficial Resolution For Heel Spur

Overview
Although a heel spur is often thought to be the source of heel pain, it rarely is. When a patient has plantar fasciitis, the plantar fascia pulls on the bottom of the heel bone. Over time this can cause a spur to form. Heels spurs are a very common x-ray finding, and because the heel spur is buried deep in soft tissue and not truly in a weight bearing area, there is often no history of pain. It is important to note that less than one percent of all heel pain is due to a spur. but frequently caused by the plantar fascia pulling on the heel. Once the plantar fasciitis is properly treated, the heel spur could be a distant memory.
Causes
A bone spur forms as the body tries to repair itself by building extra bone. It generally forms in response to pressure, rubbing, or stress that continues over a long period of time. Some bone spurs form as part of the aging process. As we age, the slippery tissue called cartilage that covers the ends of the bones within joints breaks down and eventually wears away (osteoarthritis). Bone spurs due to aging are especially common in the joints of the spine and feet.

Symptoms
The following symptoms are typical of heel spur. Stabbing pain when treading on the area affected. Dull, irregularly occurring pains in the heel area also without exerting pressure (e.g. in a reclining position) Pain when taking the first steps in the morning (after lying or sitting down for an extended period, especially in the morning) Occasional swelling in the ankle area. For the lower heel spur, extreme sensitivity at the tendon attachment (laterally in the lower heel area) For the upper heel spur, extreme pressure sensitivity of the Achilles tendon, primarily at approximately ankle height.
Diagnosis
Because the diagnosis of heel spurs can be confused with tarsal tunnel syndrome (as described earlier), most surgeons advocate performing a tarsal tunnel release (or at least a partial tarsal tunnel release) along with the plantar fascia release. This surgery is about 80percent successful in relieving pain in the small group of patients who do not improve with conservative treatments.
Non Surgical Treatment
Heel pain may be associated with a heel spur, however the heel pain is usually due to plantar fasciitis, rather than a heel spur, so treatment is usually directed at the plantar fasciitis itself. Treatment usually involves application of ice to reduce pain and inflammation, special stretching exercises, and pain-relieving or anti-inflammatory medicines. Night splints or orthotics may be recommended. It may help to avoid the activities that aggravate pain, such as long walks and running. Surgery is very rarely recommended and only after other measures fail.
Surgical Treatment
In a small number of cases (usually less than 5 percent), patients may not experience relief after trying the recommendations listed above. It is important that conservative treatments (such as those listed above) be performed for AT LEAST a year before considering surgery. Time is important in curing the pain from heel spurs, and insufficient treatment before surgery may subject you to potential complications from the procedure. If these treatments fail, your doctor may consider an operation to loosen the plantar fascia, called a plantar fascia release.
Tips On How To Treat Heel Spur
_a_preliminary_experience/links/0278c3000cf2c6a3a06f2d5c/preview.png)
Overview
When the body is under stress or constent inflammation it will deposit calcium to our bones. This added 'bone growth' is designed to relieve the added stress/pressure to our connective tissue. In the case of a heel spur, added calcium to the heel bone (calcaneus). It usually forms at the bottom underside of the heel bone where the plantar fascia attaches. This calcium deposit forms over a period of many months. Heel bones can very in shape and size from person to person. An irregular shape heel (calcaneus) can cause the tissue to twist (plantar ligament and Achilles tendon) or a smaller heel bone will put additional stress on tendons and ligaments.
Causes
Each time we take a step forward, all of our body weight first rests on the heel of one foot. As our weight moves forward, the entire foot begins to bear the body's weight, and the foot flattens and this places a great deal of pressure and strain on the plantar fascia. There is very little ?give? to the plantar fascia, so as it stretches only slightly, it pulls on its attachment to the heel. If the foot is properly aligned this pull causes no problems. However, if the foot is ?pronated?(the foot rolls outward at the ankle, causing a break down of the inner side of the shoe), the arch falls excessively, and this causes an abnormal stretching of the relatively inflexible plantar fascia, which in turn pulls abnormally hard on the heel. The same pathology occurs with ?supination? (the rolling inward of the foot, causing a break down of the outer side of the shoe). Supinated feet are relatively inflexible; usually have a high arch, and a short or tight plantar fascia. Thus as weight is transferred from the heel to the remainder of the foot, the tight plantar fascia hardly stretches at all, and pulls with great force on its attachment to the heel. In both cases, the abnormal stress placed on the attachment of the plantar fascia to the heel usually causes pain, inflammation, and possibly swelling. If this process continues, the plantar fascia partially tears away from the heel. The body will fill in this torn area with calcium; eventually it becomes bone, and a heel spur results.

Symptoms
An individual with the lower legs turning inward, a condition called genu valgus or "knock knees," can have a tendency toward excessive pronation. This can lead to a fallen arch and problems with the plantar fascia and heel spurs. Women tend to suffer from this condition more than men. Heel spurs can also result from an abnormally high arch. Other factors leading to heel spurs include a sudden increase in daily activities, an increase in weight, or a thinner cushion on the bottom of the heel due to old age. A significant increase in training intensity or duration may cause inflammation of the plantar fascia. High-heeled shoes, improperly fitted shoes, and shoes that are too flexible in the middle of the arch or bend before the toe joints will cause problems with the plantar fascia and possibly lead to heel spurs.
Diagnosis
Diagnosis is made using a few different technologies. X-rays are often used first to ensure there is no fracture or tumor in the region. Then ultrasound is used to check the fascia itself to make sure there is no tear and check the level of scar tissue and damage. Neurosensory testing, a non-painful nerve test, can be used to make sure there is not a local nerve problem if the pain is thought to be nerve related. It is important to remember that one can have a very large heel spur and no plantar fasciitis issues or pain at all, or one can have a great deal of pain and virtually no spur at all.
Non Surgical Treatment
There are various ways to treat heel spurs. The first is to rest and apply ice to the afflicted area. Shoe inserts and night splints can also treat plantar fasciitis, and in turn, heels spurs. Unless you have stomach sensitivities, you may want to consider taking over-the-counter anti-inflammatory medication such as naprosyn to lower the swelling. A physical therapist can recommend gentle exercises and stretches to relax the tissue around the heel bone to relieve the tension. Even with these treatments, a stubborn heel spur may not go away. A physical therapist may decide to inject cortisone into the area to decrease inflammation, but that can cause other problems such as plantar fascial rupture and fat pad atrophy. Extracorporeal shock wave therapy is also an option, which uses energy pulses to apply microtrauma around the heel spur. Surgery is also an option but is not suggested unless the heel spur lasts more than a year. To prevent heel spurs from returning, shoe inserts can relieve the pressure on the plantar fascia. Also continue the recommended stretches and exercises.
Surgical Treatment
Approximately 2% of people with painful heel spurs need surgery, meaning that 98 out of 100 people do well with the non-surgical treatments previously described. However, these treatments can sometimes be rather long and drawn out, and may become considerably expensive. Surgery should be considered when conservative treatment is unable to control and prevent the pain. If the pain goes away for a while, and continues to come back off and on, despite conservative treatments, surgery should be considered. If the pain really never goes away, but reaches a plateau, beyond which it does not improve despite conservative treatments, surgery should be considered. If the pain requires three or more injections of "cortisone" into the heel within a twelve month period, surgery should be considered.